
COMMENT Imagine 10 jumbo jets crashing every week for a whole year or the entire population of Petaling Jaya dying every year. That is between 210,000-440,000 number of deaths occurring due to medical errors in the United States annually based on a report from the Institute of Medicine (2013). Healthcare in America is failing.
Ironically, America has the largest private healthcare system in the world and spends more than any other country for both private and public healthcare system at US$2.8 trillion. Its spending on the healthcare system a year alone is larger than the whole economy of the United Kingdom at US$2.6 trillion or France at U$2.7 trillion. If there are no changes with the way we do things, we might be another America. So, how are we faring?
Ageing population and measuring healthcare performance
By the year 2030, Malaysia’s population will be as old as the ageing Japan. Asia and Malaysia specifically has one of the fastest ageing population in the world. According to Singapore-based Asia Pacific Risk Center (APRC), the swelling ranks of the elderly will cost the region US$20 trillion in healthcare by 2030.
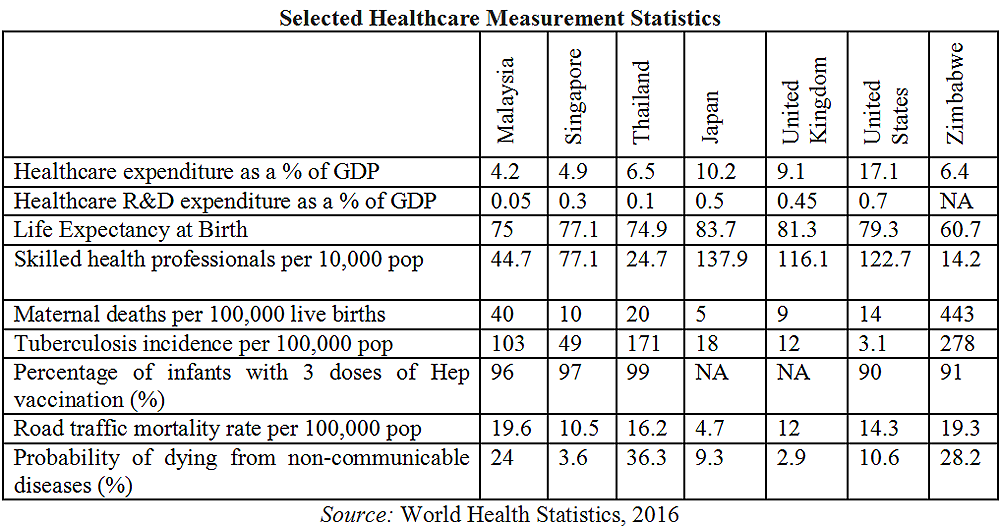
Japan spends 8 percent of its GDP on healthcare; where 80 percent of the expenses is funded by the government while Malaysia lags behind at 4.4 percent and 52.4 percent respectively. The total expenditure for both public and private healthcare is at RM50.3 billion; where Operational costs itself takes up 93 percent of the pie and only 7 percent is allocated for Development.
The GDP percentage spent on healthcare ranks Malaysia at number 156 in the world. Majority of Malaysians go to public healthcare facilities. Seventy-five percent of Malaysians seek in-patient treatment and 90 percent of Malaysians seek out-patient treatment at public facilities. Despite that, the government spends only 52.4 percent for total healthcare expenses.
This indicates two things: the far higher cost of private facilities and the affordability for the public majority to go for private healthcare.
Trying to summarise healthcare in one article is a mammoth task. The healthcare system is very complex, as it has many indicators with different expectations. This includes patients, doctors, healthcare providers, the supply chain, agencies that regulate healthcare activities, and also the government.
How do we measure the healthcare of a nation? An effective performance measurement system is essential in ensuring that we do not follow in America’s footsteps. A monitoring plan that can ensure continuous improvement in quality, effectiveness, accountability and, most importantly, affordability. The measure must also cover holistic aspects of healthcare from patient satisfaction, healthcare professionals’ efficiencies, utilisation, clinical quality, equipment, technology and financial performance.
How do we measure performance? If affordability is a measure, the cost of birthing in a hospital, in the UK and Australia with 2.6 days stay is at a one month median wage versus 3 months median wage in Malaysia. The cost of birthing is intentionally chosen as an example to be mentioned because pregnancy and childbirth is the number one cause of hospitalisation at 19.9 percent for combined public and private hospital. (Health Ministry, 2016)
Profit, subsidy or a government’s responsibility
There is an ongoing debate whether healthcare is a personal responsibility or the government’s responsibility. It is easy to accuse individuals of not really taking care of their health and that the government has done their level best in ensuring that facilities are in place. However, a person with the utmost healthcare awareness will not be able to do much if public conditions are not set up to a reasonable standard.
The government has a responsibility to ensure that our water is clean, we have a proper immunisation programme, healthy food and accommodation are affordable, and other environmental issues and surroundings are in the best condition.
Another discussion is whether the healthcare expenditure by the government is a form of subsidy or a form of the government discharging its responsibility. If we are to agree that it is one of the government’s major responsibilities, we should start correcting the term used to label healthcare spending.
I find it irresponsible that in the Pemandu’s Subsidy Rationalisation Labs, healthcare is tagged as an item to be rationalised under the subsidy programme. Such identification can be deemed as a policy attitude towards healthcare - that healthcare is a subsidy and not an investment. This will have an unhealthy effect towards healthcare.
By agreeing that healthcare is the government’s responsibility, we need to begin addressing more related issues as to the privatisation, the cost of medicine and services, the human capital and facilities, the third party administrators and also exploring other successful models implemented by other countries and subsequently identifying a way forward.
Privatisation of healthcare and profiteering private hospitals and GLCs
The Malaysian government in 1983 under then-prime minister Dr Mahathir Mohamad introduced privatisation policies which allow the private sector to play a greater role in taking away the government’s responsibilities in both healthcare and education. Healthcare has exhibited ever increasing costs since then.
Private hospitals that were run by non-profit organisations or religious organisations are now increasingly run by profit-oriented private hospitals. The idea is simple - the rich can afford private hospitals and this would reduce the traffic at government hospitals providing better services for the poorer patients.
Privatisation didn’t stop here; in 1993 the pharmaceutical services under the Health Ministry were privatised. Renong back then was awarded an exclusive long-term contract to supply medicines and supplies, subsequently doubling government spending for that provision the following year.
Instead of stopping privatisation, other support services such as laundry and linen, clinical waste management, cleaning, facility engineering and maintenance were then privatised three years later in 1996. Within a year, the cost of these services jumped to RM450 million from RM140 million.
As a result of privatisation, highly qualified and experienced doctors flocked to the private sector. Within twenty years the private sector held two-thirds of the total number of medical, surgical consultants, and specialists. Brain drain. Eventually the waiting time and quality of service in government hospitals deteriorated significantly. Some have experienced tragedies where relatives met their death due to late diagnosis or late treatment.
As reflected earlier, the cost for healthcare in private hospitals is very high. As an example, the maternity charges in Class 1 of a public hospital is RM800 which is a fraction of the cost in the private sector; which averages between RM3,500-RM6,000.
Recently, the cost of medicine has also risen sharply due to the implementation of the Goods and Services Tax (GST). In the private sector, the GST cost is transferred to the patients as it is not absorbed by private healthcare institutions.
We need to find the real cost of healthcare. Why are there Approved Permits for medicines? Profiteering must not be allowed especially by large health conglomerates, government-linked companies (GLC) like Sime Darby, Pantai, Khazanah, KPJ and others that account for more than 40 percent of private hospital beds.
The consequences of privatisation in the healthcare sector also calls for an urgent review of the privatisation policy. The government is wearing three hats, as the public healthcare provider, regulator, and as also an investor in profiteering healthcare which comes with clear conflict of interests.
Insurance supply over demand and the third party administrators’ expenses
The mandate in privatising healthcare is to distribute the burden of healthcare to the private sector. At the same time a financial model needs to be established to bear the cost and the insurance industry has done well to do so. It is estimated that the cost to insure every Malaysian at a minimum premium to cover hospitalisation costs would be at RM30 billion per year.
Over the years, the number of insurance policy holders has increased and more private hospitals have been built. With the creation of such supply versus demand, the cost of healthcare should logically be reduced. However, this has not been the case. In the past recent years, a sharp spike in the cost of healthcare services and the price of medicine can be observed clearly. New artificial demands have been created.
Over-investigations, over-treatments, and in some cases unnecessary clinical investigations are being performed at private hospitals. This practice has resulted in an offset of the supply.
There is also a need to review the high fees charged by our specialists. On average from a standard hospitalisation bill, the ratio between the fees by the hospital which includes medical, equipment cost, disposables and nursing, is at 60 percent, while the remaining fees would be from the specialist. Their fees are governed by the 13th Fee Schedule which is urgently in need of a review.
Like any other industry, the cost of healthcare is also increasing unnecessarily due to the existence of this industry’s middle-men, termed as the Third Party Administrators (TPA) or sometimes called the Managed Care Organisations (MCO). What they do is that they provide interface administration between medical providers, corporations, and the insurance companies.
They assist in processing claims, corporate and retail policies and also financial facilities. Their major revenue is in the form of fees or commissions on premium, which is standardised by the Insurance Regulatory Development Authority (IRDA). Most Malaysians are unaware of the extra premium charged by insurance companies for TPA services.
Regulations can be enforced by amending and including such provisions in existing Acts such as the Private Healthcare Facilities and Services Act 1998 (PHFSA). There are at least 30 TPAs/MCOs currently active in the country.
Malaysia’s healthcare human resources and facilities
According to the Health Ministry (2016), we have a total of 46,491 doctors in public and private hospitals; which gives us a ratio to population of 1:656, dentists at 1:4,775, pharmacists at 1:2,900, opticians at 1:9,578 and optometrists at 1:19,053. The Eleventh Malaysia Plan (2016-2020) calls for a ratio of 1:400 which means a target of 75,000 doctors by 2020.
Do we have enough training hospitals and future undergraduate doctors to achieve that? This means 28,509 new qualified doctors within the next four years.
The Health Ministry however is saying that there is an inadequacy of infrastructure to absorb graduating trainees for internships and housemanships. As such, new medical course freezes will be extended. This is indirectly saying that we do not have enough hospitals.
At the moment there are 143 public hospitals with 41,389 beds and 183 private hospitals with 12,963 beds. As 75 percent of our population choose to go to public hospitals, this means one public hospital would need to serve 157,342 Malaysians while one private hospital would need to serve 40,983 Malaysians.
There are now only 44 training hospitals. The lack of training hospitals is translated as an additional year that new doctors would have to spend before they can obtain a placement. The existing doctors who are stretched thin with the heavy workload would also not be able to provide the best of training for the apprentice doctors.
There is a way out. While building more training hospitals, we can revisit the regulation and allow trainees to do training overseas provided by universities that must be certified to conduct the training by the Education Ministry. Rural clinics can also be upgraded into mini hospitals with qualified doctors. This will increase placement position for trainees and doctors.
I have always advocated minimum wage and a bigger pie for the working force. Despite the size of the profit in healthcare, the money that goes to the salaries of our public doctors is a small proportion. Malaysia’s private sector healthcare’s EBITDA/Revenue percentage is approximately at 35 percent while Wages/Revenue is at 20 percent.
If we take a look at a developed nation as a benchmark, we can see that in Australia it is at approximately 12 percent EBITDA/Revenue and 45 percent Wages/Revenue.
Affordable Care Act and non-profit hospitals
The South Korean government did very well when they opted to promote that prevention is better than cure. In the long run, it has been proven to be a cost effective solution. The South Korean government will absorb full medical costs for its citizens provided that they do annual medical check-ups without fail.
There are also other options that can be explored such as social hospitals, where non-profit organisations run hospitals in government provided buildings. A new Act can also be drafted that can be literally labelled as the ‘Affordable Care Act’ which obligates the government to provide affordable healthcare. A measure of correlating insurance premium costs to income can also be introduced to ensure that every Malaysian citizen can afford it.
Indonesian reformists organisation Muhammadiyah’s main activities are in religion and education. Some of its schools are also open to non-Muslims. At the moment there are 5,754 schools under Muhammadiyah. Their latest venture is running non-profit medical clinics and hospitals. Today, they own several hundreds of medical clinics and hospitals in Indonesia.
Considering that 19.9 percent of all hospitalisations are related to pregnancy, we can start off with the establishment of a chain of Maternity and Paediatric Hospitals priced at the midpoint. These hospitals will provide no-frills services with wide accessibility. We can envisage a chain of hospitals in normal shoplots. The hospitals must be operated by non-profit organisations or cooperatives.
Karnataka, a state in the south western region of India is leading the way for affordable healthcare when it introduced the Yeshasvini Health Scheme, a scheme for the rural masses to access quality healthcare at only RM0.30 (5 Rupees) per month. The scheme provides free outpatient consultations and 1,700 different types of operations entirely free of cost!
Within seven months of the scheme launch, over 5,000 farmers had various types of operations and 23,500 farmers had outpatient medical consultations.
Healthcare is a collective obligation
According to the State of Households II Report released in Aug 2016 by Khazanah Research Institute's (KRI), a nutritionally adequate diet is beyond the reach of many Malaysians particularly in urban areas and after taking other living expenses into account. This is bound to have a causal effect on the state of healthcare.
The above reflects that there are other non-direct entities that affect healthcare. Healthcare must not be the sole responsibility of the Health Ministry, but a collective responsibility of every Malaysian.
The collective payment of income taxes, real property gain taxes, goods and services taxes, road taxes and other funds collected from the society, must be beneficial for the people. The money collected by the government must be transferred back to the government’s two primary obligations - health and education.
The budget must be allocated to fund medical activities and programs. This will eventually bring about many benefits for the government, ensure continuously healthy and productive labour in the country, subsequently contributing to the nation’s economy.
Moving forward, payment for doctors should not be on a fee for service basis which will avoid over-investigation and over-treatment. Income disparity between the public sector, healthcare personnel and the private sector must be narrowed. It is important that we invest in more public healthcare facilities by doubling our doctors, hospitals, and teaching hospitals within the next ten years.
Privatisation must be reviewed, a national healthcare insurance for the poor must be set up, a cost reduction review of the complete healthcare supply chain, the introduction of non-profit hospitals, a national healthcare performance measurement system and more health awareness programmes are required.
I have always been and will always be a strong proponent of the notion that the government is responsible to provide adequate healthcare and education as both are basic fundamental rights necessary in creating an advanced society. A healthy and educated society is the backbone of any successful country. Both are important investments by the government.
A complete holistic revisit for the healthcare system and industry, and a healthcare performance measurement are pivotal for our future. Something needs be done urgently, fundamentally. Let’s get our act together or we will be doomed to fail.
ANAS ALAM FAIZLI holds a doctorate in Business Administration. He is a construction and an oil and gas professional, the author of ‘Rich Malaysia, Poor Malaysians’ and tweets at @aafaizli